What is a sleeve gastrectomy operation?
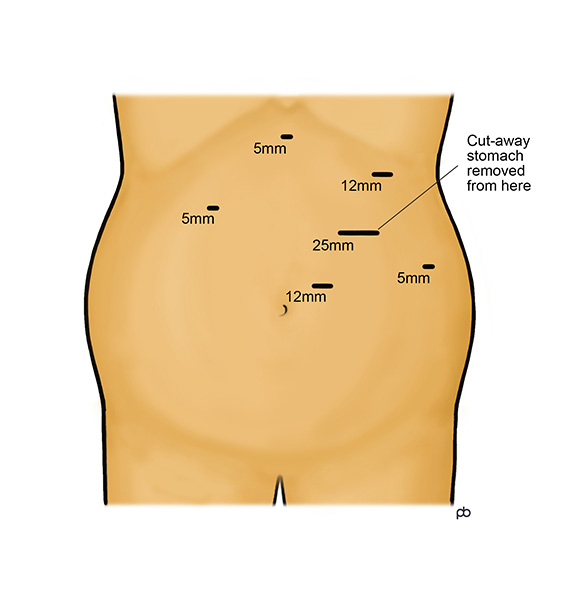
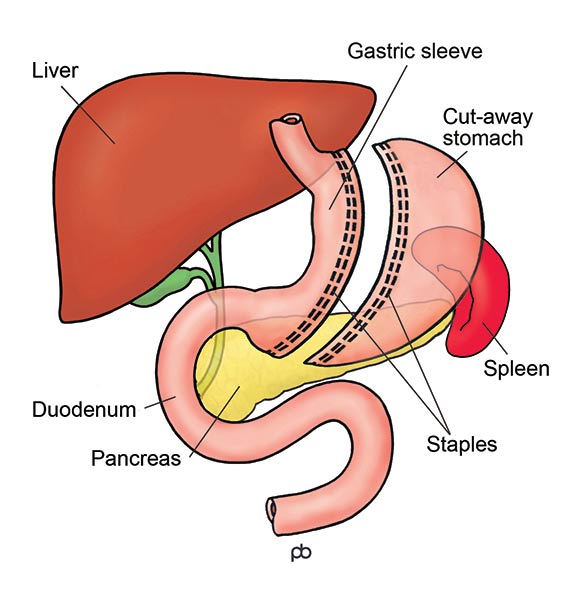
The sleeve gastrectomy operation is done by laparoscopy (keyhole surgery) under general anaesthesia in Leeds. It takes 1-2 hours. The stomach is a large sack that has a capacity of about two pints. Surgical staplers are used to change the stomach from a sack into a thin narrow tube. Surgical staplers are special surgical instruments that cut and seal the walls of the stomach simultaneously. The stapler is coated with a special material, called buttressing, to increase strength and reduce bleeding. During the operation, a special tube called a calibration bougie is passed from your mouth into your stomach. The bougie guides the stapling so that the sleeve is of the correct size. The cut-away part of the stomach is removed from your abdomen through one of the keyhole cuts that is enlarged slightly.
How does a sleeve gastrectomy work?
The gastric sleeve gives you a feeling of fullness after eating a small meal. Also, it controls your appetite so you do not feel hungry until it is time for the next meal. These effects happen because the gastric sleeve reduces the working size of your stomach. This is called the restrictive effect of operation. Also, there are changes in the levels of several hormones that control your hunger, fullness and blood sugar levels. These hormones are released from special cells in the lining of the small bowel and the stomach. Because of these changes in hormone levels, you can feel as if a switch has been turned off in your head. Your hunger is reduced and you feel fully quickly after eating.
How much weight can I lose with the sleeve gastrectomy?
Your weight loss will depend on your starting BMI and gender. Please remember that there are no guarantees in weight loss surgery .
If you are a woman and your BMI is less than 50, you could lose about 70% of your excess weight (%EWL). If your BMI is more than 50, the average weight loss is lower: about 50% EWL.
If you are a man and your BMI is less than 50, you could have 60%EWL . If your BMI is more than 50, the average weight loss is lower: about 50%EWL.
Weight loss takes place during the first year after the operation. After this time, weight-loss stops and you have reached your new weight. This new weight is called the plateau. You could imagine that the sleeve gastrectomy has reset a weigh-thermostat in your body. The sleeve gastrectomy helps you to maintain your new weight once you have reached your plateau.
What is the follow-up care for sleeve gastrectomy?
Lifelong follow-up is essential after sleeve gastrectomy. For the first 2 years after your operation, your follow-up will be with the hospital and with your GP. After 2 years, the follow-up will be primarily with your GP, but either your GP or you can contact us at any time for advice. You can think of the follow-up care in 3 parts: