What is the gallbladder?
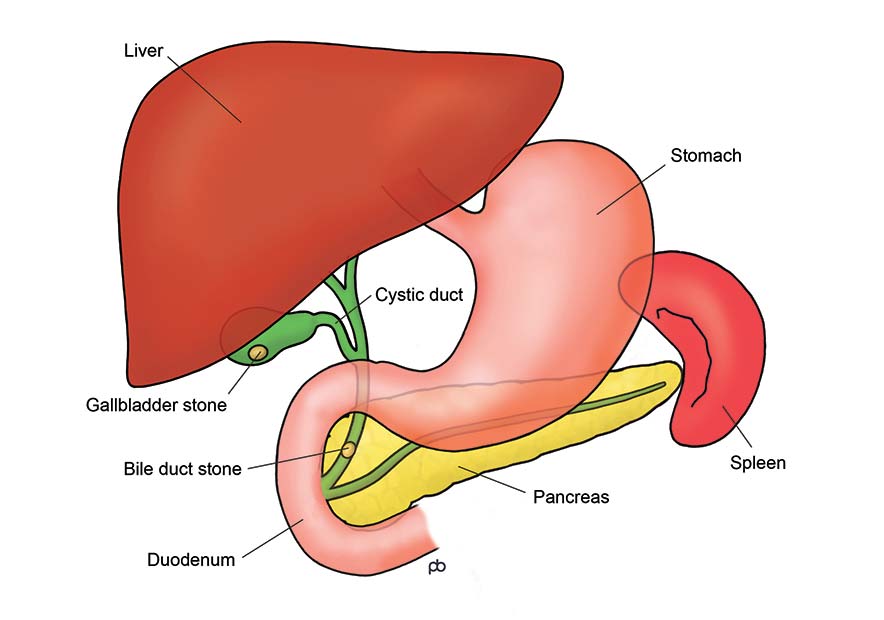
The gallbladder is a sack-like structure that is located just below your liver. The gallbladder lies beneath the lower end of the right side of your rib cage. The function of the gallbladder is to store bile, which is made in the liver and is carried to the bowel by the bile duct. The gallbladder is attached to the bile duct by a tube called the cystic duct. Bile enters and leaves the gallbladder through the cystic duct.
What is the function of the gallbladder?
The gallbladder stores bile that is made by the liver, and it releases the bile into the bowel after a meal. Bile is important for digestion. But, the gallbladder does not serve a vital function in the human body: you can live easily without your gallbladder. After removal of the gallbladder, bile flows directly into the bowel. Removal of the gallbladder does not usually cause any digestive problems. There is no restriction on food after a gallbladder operation. Digestion continues to take place as it did whilst the gallbladder was in place. Most people can eat more comfortably after removal of a gallbladder that contained stones. But occasionally, you can get diarrhoea because of poor absorption of bile acids from the bowel after removal of the gallbladder.
Why do stones form in the gallbladder?
Gallbladder stones – called gallstones – develop because of deposition of crystals of cholesterol, bile pigments, calcium and other substances from bile. The crystals get deposited and enlarge to form stones when there is change in the composition of bile, or if the gallbladder does not empty properly. There are many risk factors for the formation of gallstones. The risk is higher is women than in men. The risk is increased by pregnancy, oestrogen hormone treatment, certain genetic traits, obesity and rapid weight loss. Certain blood diseases, called haemolytic anaemias, increase the risk for pigment gallstones. The composition of the gallstones does not change treatment. There is no good evidence that change in life-style can prevent or dissolve gallstones.
What problems are caused by gallstones?
Gallstones can cause many problems
How are Gallstones diagnosed?
Gallstones (gallbladder stones) are diagnosed by doing a scan of your gallbladder. Most commonly, it is an ultrasound scan. Ultrasound is an accurate test for stones in your gallbladder, but it may not detect stones that have passed into your bile duct. Stones in the bile duct are suspected if the duct appears dilated (swollen) on ultrasound scan. Also, bile duct stones may be suspected by abnormalities in blood tests (called liver function tests). The bile ducts can be checked by a special MRI scan, called called MRCP (Magnetic Resonance Cholangio-Pancreaticography).
What is the treatment of gallstones?
The treatment of gallstones is an operation to remove the gallbladder. The operation is done by laparoscopy (keyhole surgery) and it is called Laparoscopic Cholecystectomy. Non-surgical treatments, such as fragmentation of the gallstones by shock waves or dissolving gallstones by medicine, have low rates of success and high risk of re-formation of the gallstones. Also, removal of gallstones and leaving the gallbladder in place is not done because it is very likely that there would be further problems.
Does everyone with gallstones need an operation?
The decision about whether or not to do an operation for gallstones (gallbladder stones) depends mainly on your symptoms. You may have Symptomatic Gallstones, Asymptomatic Gallstones or Gallstones with Atypical Symptoms.
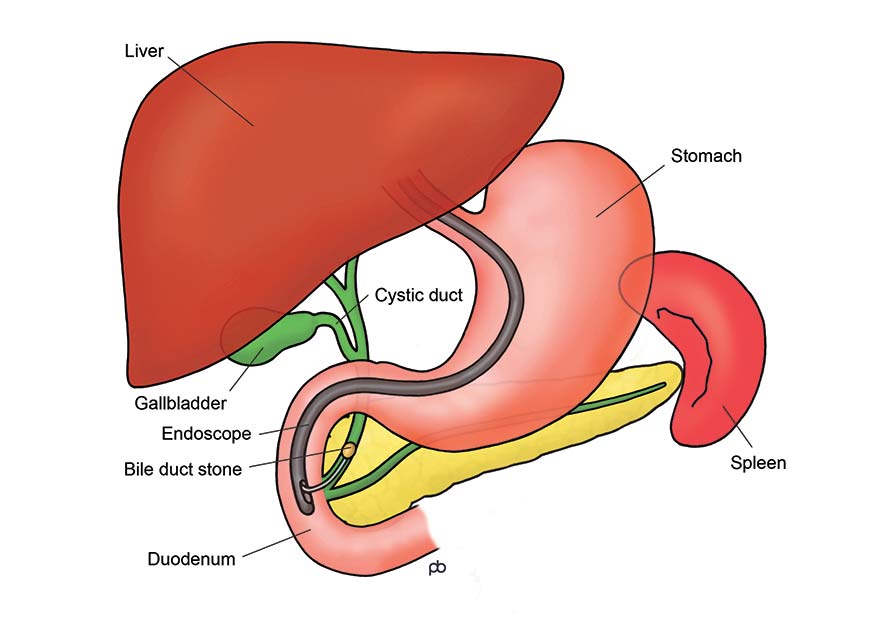
What is the treatment for stones in the bile ducts?
Stones from your gallbladder may have passed into your bile ducts. Stones can be removed from the bile duct in two ways:
What is Laparoscopic Cholecystectomy?
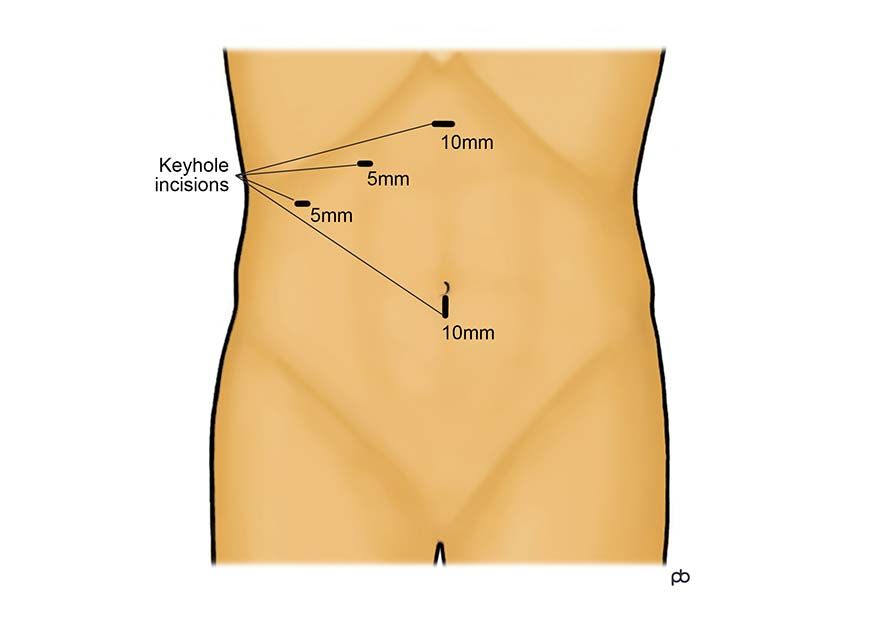
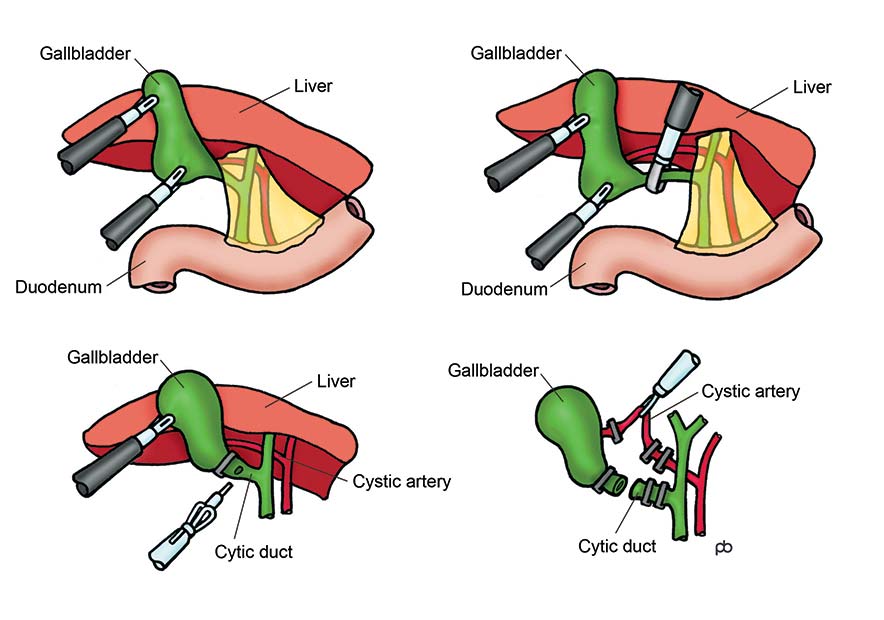
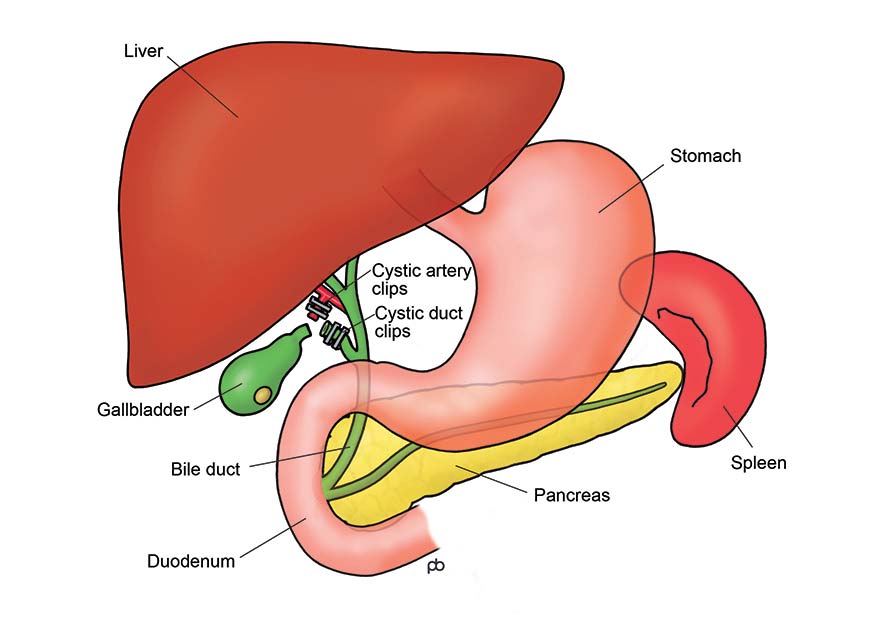
Laparoscopic Cholecystectomy is removal of your gallbladder by keyhole surgery (laparoscopy). The operation is done under general anaesthesia. Most patients can go home on the same day. Four keyhole sized cuts are made on your abdomen (tummy). The gallbladder is separated from the liver, and the blood vessels to the gallbladder are divided securely. The gallbladder is attached to the bile duct – the tube that carries bile from the liver to the bowel – by another tube called the cystic duct. In order to remove the gallbladder, the cystic duct is cut and sealed by surgical clips or stitches. The gallbladder is then placed in a special bag and removed via the keyhole at your bellybutton.
What are the risks from Laparoscopic Cholecystectomy?
Most people may a straightforward recovery and serious complications are rare. But, all keyhole (laparoscopy) operations on your abdomen (tummy) carry some risks. There is some risk of excessive bleeding whilst separating (dissecting) the gallbladder from the liver. A rare but very serious risk is injury to the bile duct. This is the tube that carries bile from the liver to the bowel. Bile can leak out in to the tummy from the bile duct and cause serious infection. The treatment of bile duct injury can require endoscopy (called ERCP) and major corrective surgery. If the gallbladder is very stuck to the bile duct, then a sub-total cholecystectomy may be done. Here, a small part of the wall of the gallbladder is left on the bile duct in order to protect the duct.
Gallbladder polyps
A polyp is growth from the wall of the gallbladder. The concern is about the risk of transformation of a polyp into cancer. But, not everyone with gallbladder polyps needs an operation to remove the gallbladder. In some cases, no action is needed or periodic monitoring by ultrasound scan may be sufficient. For others, a cholecystectomy operation is advisable. The decision about whether or not to do an operation depends on several factors, such as the size, shape and numbers of polyps, symptoms and age.